 zarkam21:
zarkam21:
Check please
 zarkam21:
zarkam21:
@Ferredoxin4
 Ferredoxin4:
Ferredoxin4:
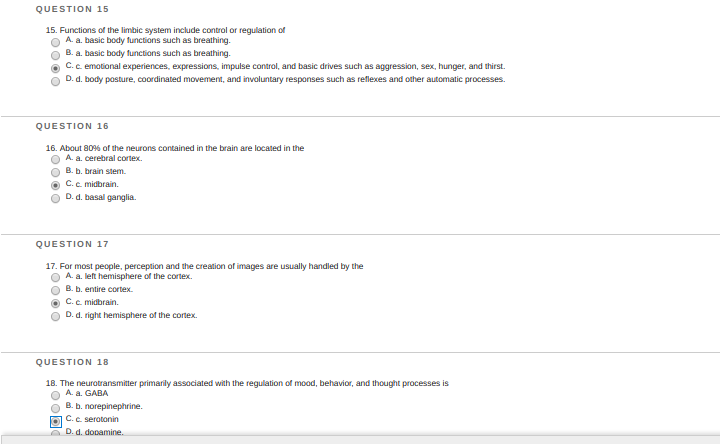
I agree with 15, I agree with 16, and 18 is correct. For 17 I'm not completely sure. Although midbrain has a core function of vision, hearing, and arousal, it also said perception as well. Also notice how it says 'for most people'. This kind of makes it sounds more like A, but once again I'm not sure.
zarkam21:
for 17, C?
Ferredoxin4:
Hm actually still thinking.
Ferredoxin4:
It would be A actually. The question is regarding about perception, and it's talking about where it's most commonly found. Perception has to do with higher order level thinking, not simply relay of sensory and motor messages. I'd go for A.
Ferredoxin4:
If it was asking about sensation, C would be a better choice (due to the thalamus). But since it's perception, it would be the cerebral cortex, specifically left in this question.
 Ferredoxin4:
Ferredoxin4:
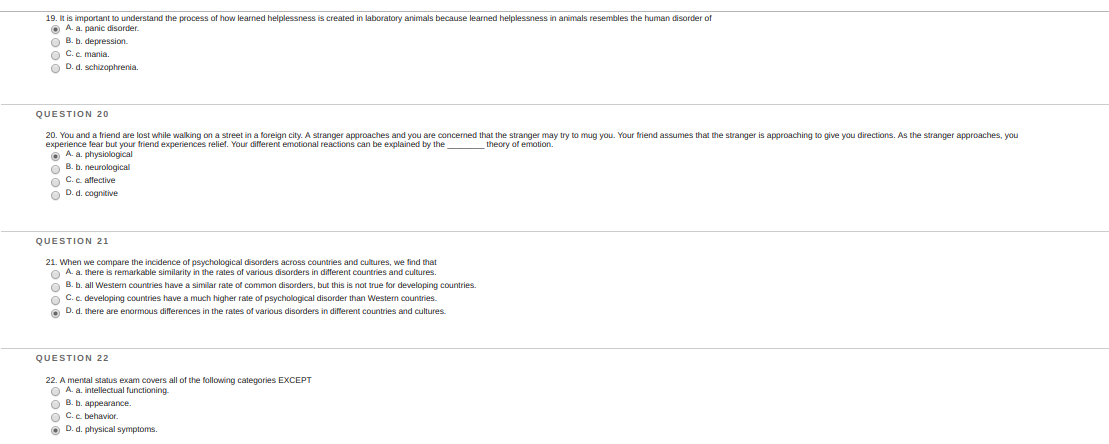
19 is A. Learned helplessness is when negative results repeatedly occur, instilling hopelessness in the individual. This leads to depression. This theory is a behavioral approach to undersanding MD. 20. There is no such thing as 'physiological theory of emotion'. It's talking about the theories of emotions: 1. Common Sense theory 2. James Lange theory 3. Cannon Bard theory 4. Schachter Singer Theory/two-factor theory 5. Facial feedback theory 6. Lazaurus Cognitive medial theory Without even thinking, you can eliminate all A, B, and C. It's only option D. I'll explain all these theories in a moment.. 21. Correct 22. Correct
Ferredoxin4:
Before discussing the theories of emotion, recall that emotion can be simply characterized as pleasant and unpleasant, and then broken down. These theories will attempt to explain the basis and foundation of emotion, and what gives us specific emotions: 1. Common sense theory Stimulus→Conscious emotion→ANS arousal (ie snarling dog→fear→sympathetic response, fast breath, etc) 2. James-Lange Theory Stimulus→ANS arousal→conscious emotion (ie snarling dog→sympathetic response→fear) 3. Cannon Bard Theory Stimulus→Subcortical stimulations→ANS arousal AND conscious emotion simultaneously (ie snarling dog→subcortical stimulation inside brain→sympathetic AND fear 4. Schachter-Singer/Two-factor theory Stimulus→ANS arousal AND cognitive labelling→conscious fear [congitive labelling means that you think about what is going on] (ie snarling dog→individual is thinking, "Oh! It's dangerous!" and simultaneous has Sympathetic response→fear 5. Facial Feedback Theory stimulus→ANS Facial arousal→facial expression→cognitive interpretation of the face→emotion ie dog→sympathetic reactions in face→individual cries→individual says, "I'm scared!"→fear [This is the most incorrect theory and is difficult to understand, but if you see a question that has to do with facial expressions and theory of emotion, it's automatically this one] 6. Lazaurus' Cognitive Mediational Theory Stimulus→Appraisal of emotion→emotion→bodily response Dog→appraisal of threat, or the individual may say, "The dog is unleashed and snarling"→Fear→ANS sympathetic arousal All of these are very important to memorize, as they are all commonly asked questions on exams.
Ferredoxin4:
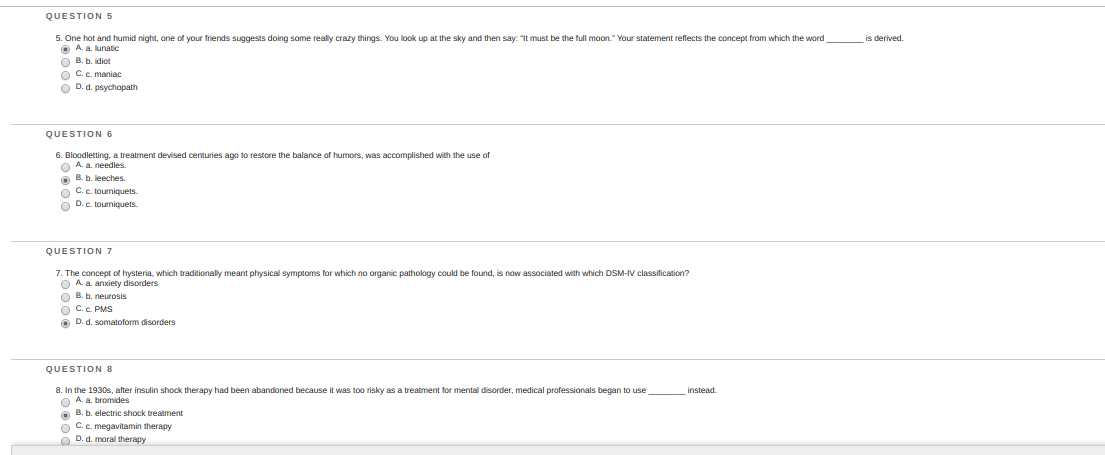
5. Lunatic is correct 6. Leeches is correct 7. Somatoform is correct 8. correct
Ferredoxin4:
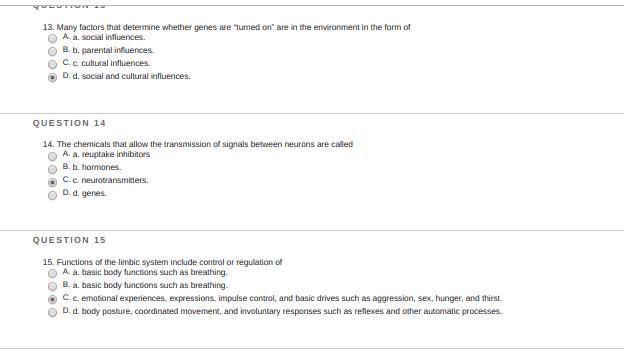
13. Correct. 14. Correct. 15. Correct
 Ferredoxin4:
Ferredoxin4:
Just noticed an error on question 16. It would be A, cerebral cortex. Recall that the cerebral cortex is used for higher order mental function. The more complex the structure is, the more neurons are there.
Ferredoxin4:
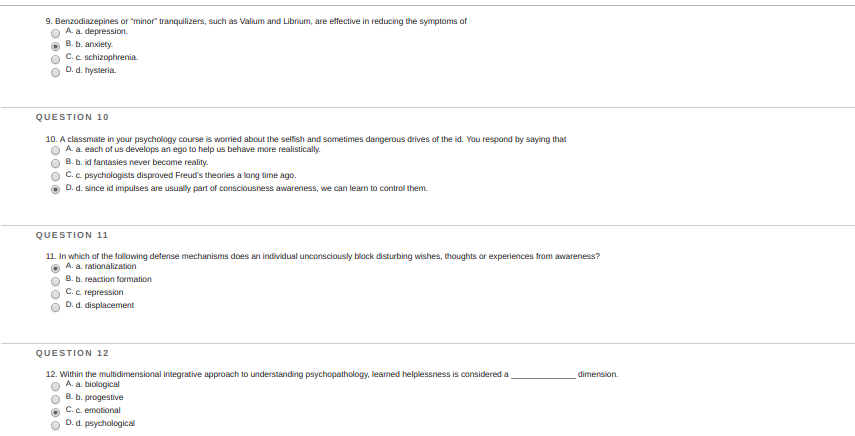
9. Correct 10. It's A. I will explain in the following response 11. It's C repression I will also explain 12. It's D, Will explain
Ferredoxin4:
10. Freud's Personality Systems--- 1. Id it is part of the UNCONSCIOUS mind, irrational, illogical, and impulsive thoughts. It works off of the pleasure principle. Pleasure Principle - immediate satisfaction without regard for consequences An easy way to remember id is: if id feels good, do id. [id=it] 2. Ego - reality, mostly conscious, rational, logical, and involves Freudian defense mechanisms. It works off of the reality principle. Reality Principle - Do it only if you can get away, and not deal with consequences. It considers the consequence. 3. Superego - moral center, makes you feel guilty/proud. It has conscience and works on Moral Anxiety Principle. Moral Anxiety Principle/Conscience - guilt is produced based on behavior.
Ferredoxin4:
11. 10 Freudian Ego Psychological Defense Mechanisms---- 1. Denial - refuse to agree (ie "I'm not smoking" even though the individual is smoking) 2. Repression - unconsciously forgetting events from conscious memory (ie "I've never been bullied!" but was bullied). Another good example would be the Tip-of-the-tongue effect. 3. Rationalization - Making excuses (I didn't eat because I wasn't hungry) 4. Projection - Projecting one's own thoughts on others (ie "I don't like her! She likes me!") 5. Reaction Formation - Forming emotional reactions opposite to bad thoughts (ie "Ha! You're ugly!" when in reality the person likes the other person) 6. Displacement - Expressing feelings on others (ie individual fired from boss, but fights with husband) 7. Regression - Returns to an infantile stage (kicks cans and soda bottles in anger) 8. Identification - Tries to identify or behave as someone else to deal with anxiety 9. Compensation - Compensating for lack of skill in one area to superior in others (An individual fails at baseball, but he puts all his hardwork in soccer) 10. Sublimination - Turning unacceptable urges to acceptable socially (ie someone who is very aggressive and enjoys killing others is serving in the military)
Ferredoxin4:
12. It wouldn't be A. I've never heard of B, progestive. The reason why it isn't C is because 'emotional' is not a dimension. Emotions are studied by almost all approaches (psychodynamic, humanistic, behavioral, cognitive, etc.). The last one is D. I would've personally gone for Behavioral approach, but it wasn't an option.
 Ferredoxin4:
Ferredoxin4:
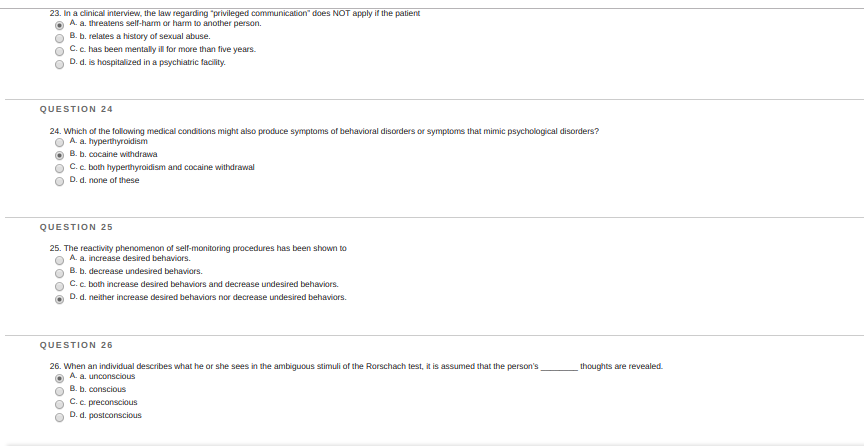
23. Haven't studied this as much, but Option A makes the most sense. Correct 24. Cocaine withdrawal is defiintely correct, but I'll check on hyperthyroidism as well. I'd say C and I'll explain 25. I'd go for C and I'll explain 26. Correct.
Ferredoxin4:
24. This was a tricky one. Cocaine withdrawal obviously can induce psychological effects. Hyperthyroidism could also mimic psychological disorders. If you didn't study the psychological impacts of hyperthyroidism, you can still answer the question. Recall that Hyperthyroidism=over production of thyroxine. An overproduction of any hormone can yield several effects, many of which of psychological. Hyperthyroidism does actually increase the risk of affective psychosis, anxiety, etc.
Ferredoxin4:
25. Self-monitoring is thinking and observing your own social behavior. This would of course impact your future behavior, because the purpose of self-monitoring is to see your current behavior and how you wish to behave socially. This is why it's option C.
 Ferredoxin4:
Ferredoxin4:
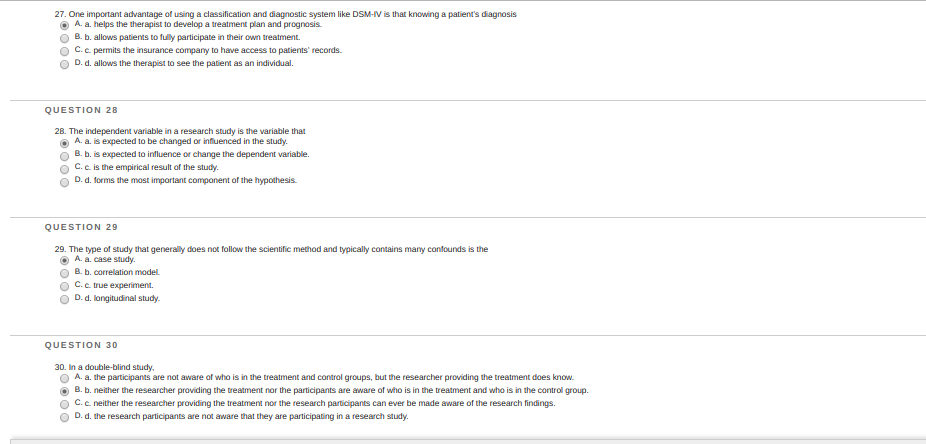
27 Correct 28 Correct 29 Correct 30 Also correct
 Ferredoxin4:
Ferredoxin4:
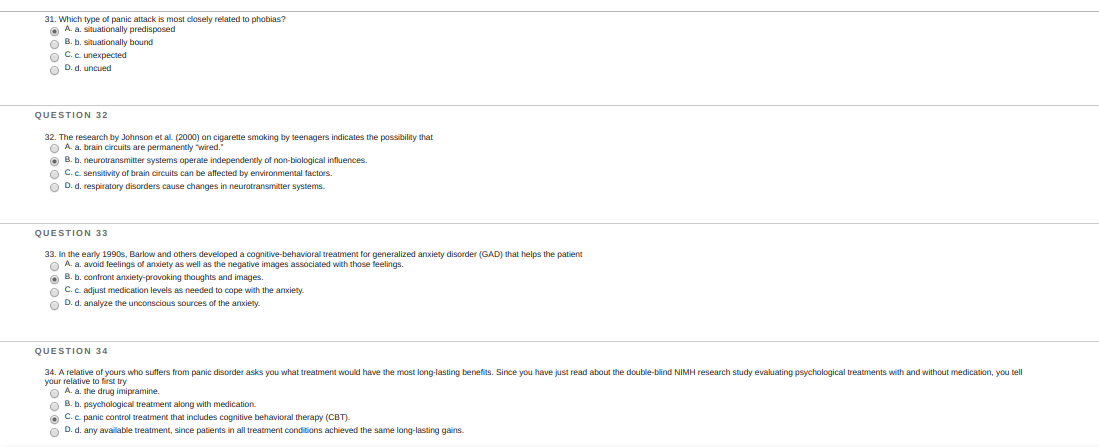
31. I'd say it's B. I'll explain 32. I'm not familiar with the Johnson study. 33. Correct 34. Correct
Ferredoxin4:
Situationally Predisposed - having the panic attacks in specific areas WITHOUT any fear of the situation. Situationally bound - having panic attacks in specific areas WITH prior fear and exposure of the situation. Unexpected and Uncued really mean what they are.
 zarkam21:
zarkam21:
These are all, jut answer when you get back thanks @Ferredoxin4
 BenLindquist:
BenLindquist:
@Tranquility
Ferredoxin4:
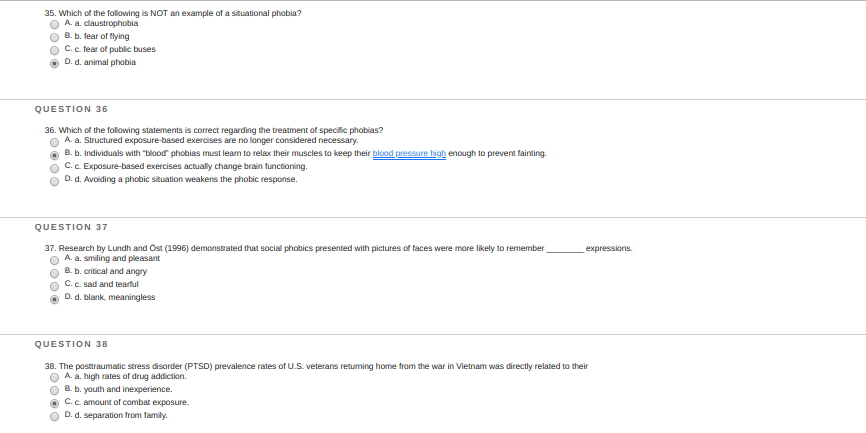
35. Correct 36. It's option C. This is known as flooding/exposure behavioral therapy. Will explain 37. It's B. This is just something you have to know by heart. Know all the experiments, including Asch, Milgram, Zimbardo, and also the famous researches. 38. I think it's A, but I'll get back on that one.
Ferredoxin4:
38. It's between A and C. I'm going for A because there were Vets that didn't participate in active warfare but had side roles but still dealt with PTSD. Also, there is a correlation between PTSD in Vietnam Vets and the use of specifically Cocaine.
Ferredoxin4:
36. Option A - incorrect because exposure therapy and systemic densitization are becoming more common treatments for phobias. Option B - The reasoning and context of the answer is wrong. Progressive muscle relaxation doesn't increase blood pressure, either. Option C - Correct. Exposure/flooding therapy would of course change brain functioning. In fact, that's the purpose of exposure therapy. Option D - Avoiding a phobic situation strengthens the phobic response. This is the logic behind exposure therapy. By exposing the stimuli, the phobic response slowly decreases.
Ferredoxin4:
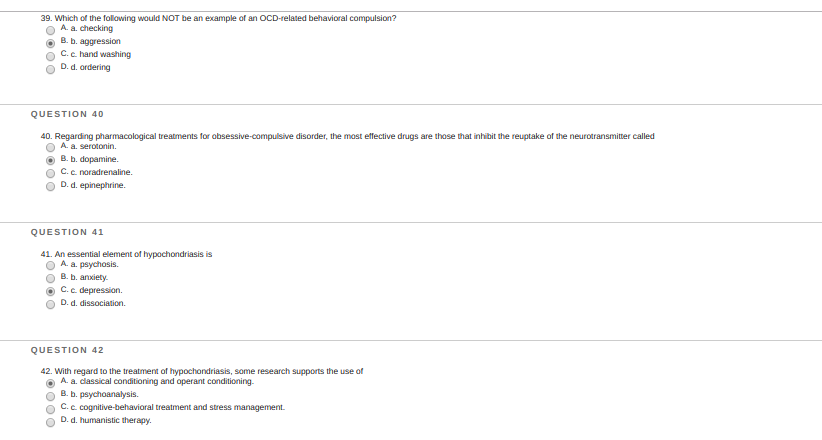
39 Correct 40. It's serotonin. OCD patients are usually given SSRIs, specifically Zoloft. There are several hints given without having to know the information. Notice how it says 'inhibit the reuptake'. This would increase the concentration of the neurotransmitter, and SSRIs do that job. Also, serotonin improves the mood and arousal, necessary for OCD patients. Dopamine is related to learning and reward pathway. This is not related to OCD. 41. It's B. Illness Affective Disorder (as per DSM 5) is where you present anxiety of a normal body process and label it as an illness (ie An individual thinks he has a tumor when it's just a callus) Depression is not related to IAD 42. C would make the most sense. IAD includes anxiety for irrational and illogical thinking. It is the irrational and unjustifiable cognition that makes the person believe he or she has a disease for a normal body process. Cognitive restructuring, therafter, is necessary to fix the issue. C would be the most reasonable option
Ferredoxin4:
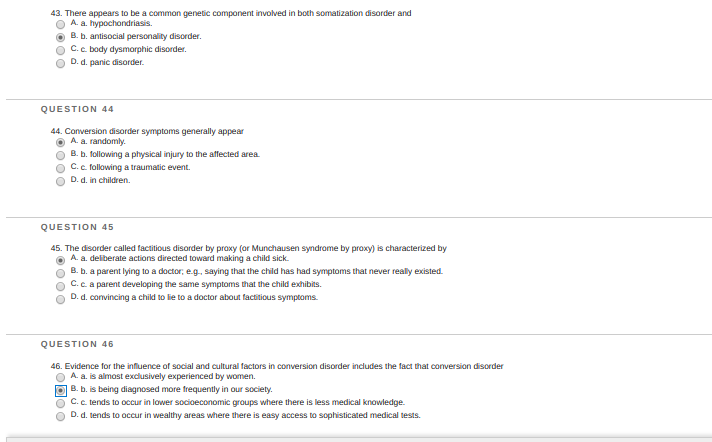
43. Haven't studied this as deeply, but I agree because the other 3 wouldn't have a genetic predisposition. 44. It's C. A common example of conversion disorder is: A father gets suddenly blind after seeing his daughter die in a car crash. 45. Correct 46. Correct
Ferredoxin4:
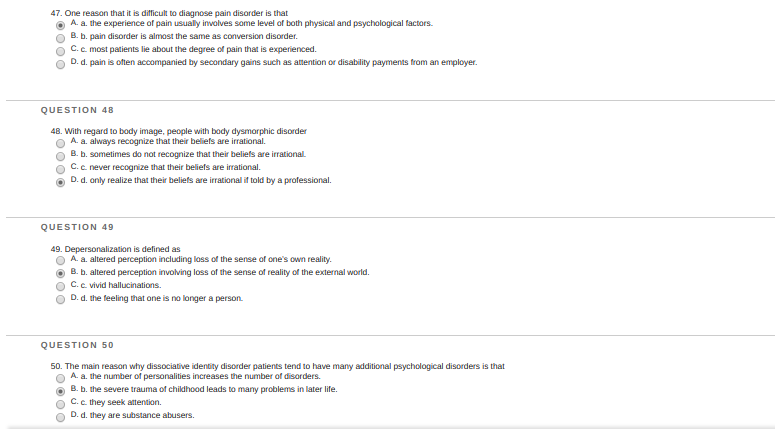
47. I agree, it could either be physiological or a somatoform disorder. 48. Option B or C. I'll get back on this one. This is why Anorexia Nervosa and Bulimia are very difficult to treat, especially Anorexia. Only 40-60% of patients diagnosed with Anorexia can recover. The rest, unfortunately, die of ventricular fibrillation and are usually young women. Bulimia is also very difficult to diagnose, because there is no change in weight and the person has both binge eating disorder AND body dysmorphic disorder. 49. Correct. 50. Correct. It could also be due to fugue which only makes it worse.
Ferredoxin4:
48. I'd go for B, because Anorexia nervosa and Bulimia aren't the only examples of BDD. There are several more, many of which the patient can recognize their beliefs as illogical.
Ferredoxin4:
\(\color{##51FF33}{\text{Originally Posted by}}\) @Ferredoxin4 Bulimia is also very difficult to diagnose, because there is no change in weight and the person has both binge eating disorder AND body dysmorphic disorder. \(\color{##51FF33}{\text{End of Quote}}\) I meant binge eating disorder and purge eating disorder.
Join our real-time social learning platform and learn together with your friends!
 Bounty:
the world keeps moving fast and I'm stuck in a time lapse all I need is a minute
Bounty:
can I get so tips on how to start my journey into semi-realism art also on how to
Bounty:
the world keeps moving fast and I'm stuck in a time lapse all I need is a minute
Bounty:
can I get so tips on how to start my journey into semi-realism art also on how to
 Strawberryluna:
Read my poem. Im not for criticism its a poem I wrote after my breakup: Youu2019ll never understand the way you made me break, I hate that I still love you
Bounty:
first poem in a min- (tittle)? one moment i'm fine I smile till my face burns I laugh till I cant breath Then I cry I wonder where I went wrong I listen to
Strawberryluna:
Read my poem. Im not for criticism its a poem I wrote after my breakup: Youu2019ll never understand the way you made me break, I hate that I still love you
Bounty:
first poem in a min- (tittle)? one moment i'm fine I smile till my face burns I laugh till I cant breath Then I cry I wonder where I went wrong I listen to
 Twaylor:
3d printing a glider (for 150 pound 5'8 person - prolly should make it for up to
Twaylor:
3d printing a glider (for 150 pound 5'8 person - prolly should make it for up to
 cullenn:
pitter patter sound of rain gently tapping my window tonight. calming, soothing, right? not for me.
cullenn:
pitter patter sound of rain gently tapping my window tonight. calming, soothing, right? not for me.

 Arriyanalol:
DON'T BUY TICKETS TO SEAWORLD i watched a documentary on seaworld and its sad wha
Arriyanalol:
DON'T BUY TICKETS TO SEAWORLD i watched a documentary on seaworld and its sad wha
 natalieee:
who else wants a job in biology? I love biomedical science and want to work with
natalieee:
who else wants a job in biology? I love biomedical science and want to work with